Knee Replacement
KNEE REPLACEMENT SURGERY
 Knee
Knee
Quality of life is never to be underestimated and when a knee problem is so debilitating that it is impossible to enjoy hobbies that are important to you like gardening or playing with your children or grandchildren, than it is crucial to seek medical help.
Fortunately, before even considering knee replacement surgery as an option, generally physicians will try to find other ways of relieving knee pain. For instance, physical therapy, medications, orthotic, knee sleeves and walking aids might be the answer to many knee pain problems including those stemming from arthritis.
However, when other treatments prove to be futile, knee replacement surgery is an option. Each year in the U.S. over 600,000 knee surgeries are performed each year, according to the U.S. Government Agency for Healthcare Research and Quality. It is estimated that this number in will increase over the next 10 years with the aging Baby Boomers.
Knee replacement surgery can be a godsend to those with painful knees as it renews the person's ability to walk, golf, play tennis and all their other favorite activities.
WHO IS A CANDIDATE FOR KNEE REPLACEMENT SURGERY?
Knee replacement is a procedure generally reserved for those who are over 60 years of age who are in relatively good health, aside from their knee pain. In fact, 72 percent of knee replacements are done on those over the age of 65. Generally, this means, they maintain a healthy weight, they do not suffer from cardiovascular problems, and they are not suffering from a terminal illness.
Active knee replacement candidates will find it comforting to know that they will be able to resume some athletics following surgery such as golf, swimming, and walking. Some knee replacement surgery recipients have even continued to play tennis and snow ski. Unfortunately, a knee prosthesis is not quite as effective as a healthy, natural knee, however it will be a great improvement over the preoperative pain and discomfort.
WHO IS NOT A CANDIDATE FOR KNEE REPLACEMENT SURGERY?
To receive knee replacement surgery, you must be a good candidate. If not, surgery could prove counterproductive. For some, knee replacement surgery is not in their best interest.
Those who are too young, with the exception of those who suffer from severe rheumatoid arthritis, should consider other types of treatment for knee pain since the artificial knee joint may need to be replaced after they have reached full growth. Unfortunately, the bone will need to be cut short to make room for the new knee joint and function and mobility is likely to be damaged during the second operation.
Those who are overweight are also not good candidates for knee replacement surgery as the natural knee is NOT designed to carry a 300 pound object. Too much weight on the artificial joint can cause it to be damaged which can cause subsequent knee problems and additional knee replacement surgeries.
Those with cardiovascular problems and with terminal illnesses are also not good candidates as the surgery may be too much for the body to handle. Also those with poor skin coverage over the knee are not good candidates as surgery could impair movement of the knee.
HOW IS KNEE REPLACEMENT SURGERY DONE?
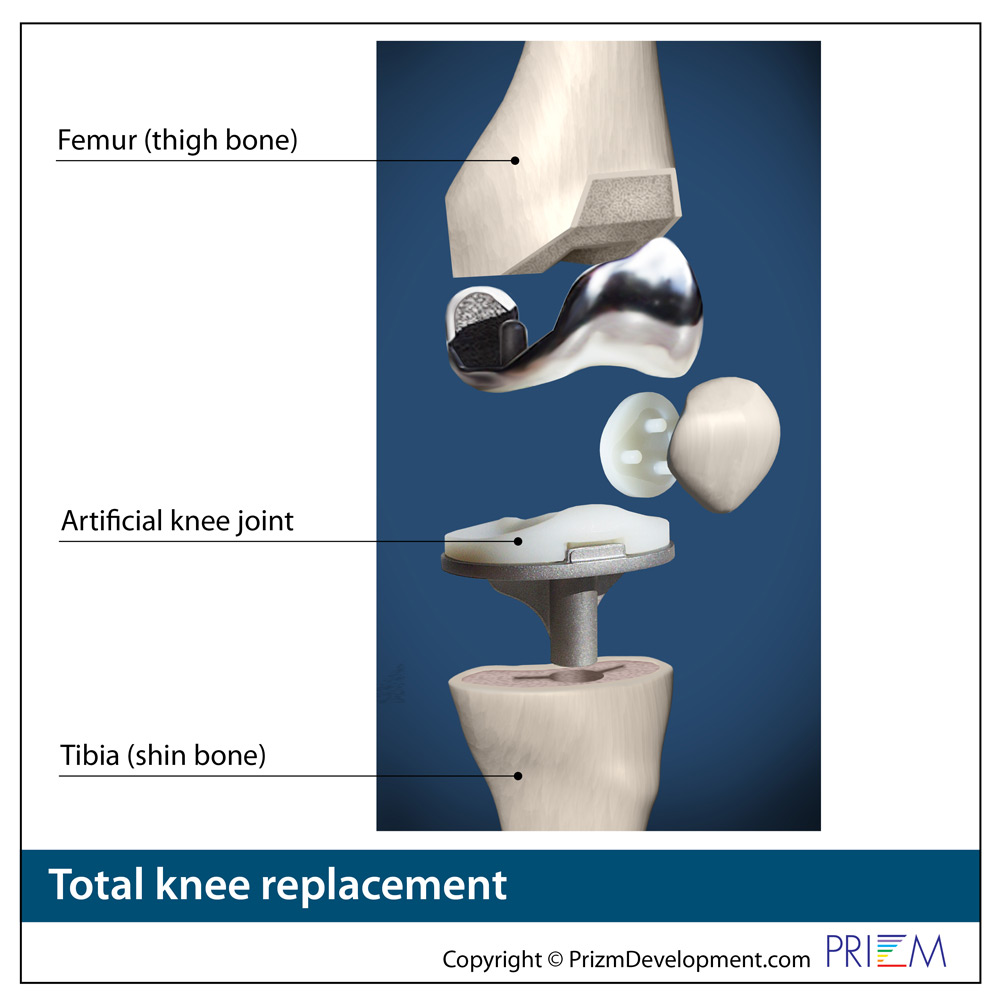
During knee replacement surgery, the patient is under general anesthesia and unconscious. The knee replacement surgery usually lasts a couple hours. The knee joint is opened up and the kneecap is moved out of the way. Doctors then, shave off the bottom of the femur and the top of the tibia and fibula bones.
Because knee replacement surgery is becoming commonplace, more knee replacement surgeries are now being done in an Ambulatory Surgery Center (ASC). These patients go home later the same day to recover in the comfort of their own home.
After the hospital stay, the patient will probably require the aid of a walker for a few days before putting full weight on the leg. Overall, full recovery can take anywhere from two months to a half year.
PARTIAL KNEE REPLACEMENT OR TOTAL KNEE REPLACEMENT?
The knee joint relates to three areas of the knee: 1. the inside part of the knee; 2. the outside part of the knee; and 3. the front of the knee under the femur (thighbone).
If the damage to the knee, and the arthritis is confined to just one part of the knee, the joint replacement surgeon may recommend a partial knee replacement for the purpose of sparing the most bone as possible during surgery.
In fact, bone sparing is the main objective of all modern knee and hip replacement surgery. The more natural bone that can be preserved during joint replacement, the better.
Sadly, many orthopedic surgeons note that too many patients receive total knee joint replacements when they only needed partial knee joint replacement. This typically is because the patient went to a joint surgeon that is not as well trained or experienced in the most advanced joint replacement techniques, and that includes the most current robotic surgery technology.
Consequently, the burden is on the patient to research the best-trained and most experienced joint replacement surgeon to assess their joint pain issue, as that will determine if they receive the optimal clinical outcome with the most bone preserved during joint replacement surgery.
 Knee
Knee
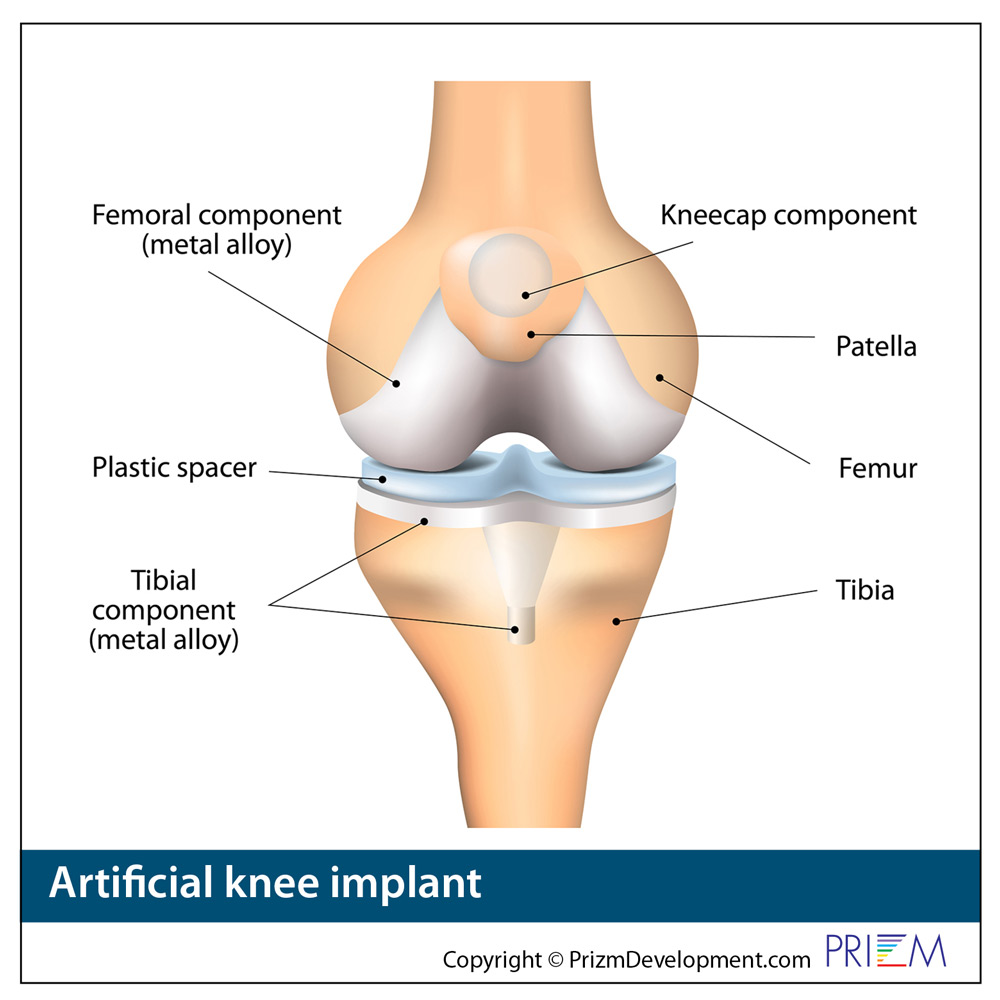
KNEE REPLACEMENT WITH AN ARTIFICIAL JOINT
Osteoarthritis is the most common reason for replacing an arthritic knee with an artificial knee joint.
Knee replacement surgery was first performed in 1968. Over the past 50 years, the procedure has greatly improved the lives of patients, enabling patients to walk and plays sports again without the limitation of pain symptoms.
Each year, there are more than 200,000 total knee replacement surgeries in the United States. About 65 percent of total knee replacements are done on women, with an average age of 68 years old. About 25 percent of all knee replacements are done on middle-aged men and women between forty-five and sixty-four years old.
Total knee replacements are one of the most successful procedures in all of medicine. It's estimated the almost 800,000 knee replacements are performed each year in the United States. It's estimated that about 4.5 million Americans are currently living with at least one total knee replacement. About 63% of the patients who receive a total knee replacement are women.
Over 10 years to 2009, total knee replacement increased by 84% in the American population. Ironically, it's not the elderly driving the large increase in knee replacement surgery. The increase is coming from younger and middle-age Americans that have lost control of their weight, and their obesity has destroyed their knees.
According to the U.S. Government's National Center for Health Statistics, women had a higher rate of total knee replacement than men. In 2010, total knee replacement was the most frequently performed inpatient procedure on adults 45 and older. The mean age for having a total knee replacement was is getting younger, from 68.9 years old in 2000 to 66.2 in 2010.
Who is a candidate for an artificial knee joint?
Total knee replacement is reserved for the patient who has not benefited from conservative treatments and whose quality of life is suffering due to the debilitation caused by knee pain. Examples include those experiencing pain at night and those who cannot perform their normal, everyday activities.
Typically knee replacement is reserved for those who are over 60 years of age who are in relatively good health. That's because the lifespan of an artificial joint is estimated to last 15 to 20 years. The goal is to have the artificial joint outlive the person.
Many times that is simply not possible because more people can benefit from joint replacement while in their 40s and 50s. This ultimately can require a complex revision surgery when the person is in their 60s or 70s when other health issues may be a complicating factor to a second surgery and a longer recovery.
Active knee replacement candidates will find it comforting to know that they will be able to resume some athletics following surgery such as golf, swimming, and walking. Some knee replacement recipients have even continued to play tennis and snow ski. Unfortunately, a knee prosthesis is not quite as effective as a healthy, natural knee, however it will be a great improvement over the preoperative pain and discomfort.
Who is not a candidate for artificial knee surgery?
As mentioned before, to receive knee replacement surgery, you must be a good candidate. If not, surgery could prove counterproductive.
For some, knee replacement surgery is not in their best interest. Those who are too young (except for those who suffer from severe rheumatoid arthritis) should consider other types of treatment for knee pain, since after 15 or 20 years, the prosthesis will need to be replaced.
Unfortunately, the bone will need to be cut short to make room for a new prosthesis, and function and mobility is likely to be damaged during the second operation.
Those who are overweight are not good candidates, as the prosthesis (just as the natural knee) is designed to carry a weight in proportion to the person's body. Too much weight on the prosthesis can cause it to be damaged, and subsequent knee surgeries will be necessary. Those with cardiovascular problems and terminal illnesses are also not good candidates, as the surgery may be too much for the body to handle. Also, those with poor skin coverage over the knee are not good candidates, as surgery could impair movement of the knee.
How is artificial knee replacement performed?
During knee replacement surgery, you will be under general anesthesia meaning you will be asleep and without pain during the entire procedure, which usually lasts a few hours.
The knee is opened up and the kneecap is moved out of the way. Doctors then, shave off the bottom of the femur and the top of the tibia and fibula bones. The prosthesis is then glued to the bones with special, surgical cement. The knee is then sutured back together and drainage tubes are used to prevent clogging.
Usually, a hospital stay for knee replacement surgery lasts between four and five days. During your time at the hospital, your leg will be attached to a device called Continual Passive Movement (CPM), which will move your knee to prevent stiffness. After the hospital stay, the patient will probably require the aid of a walker for a few days before putting full weight on the leg. Overall, full recovery can take anywhere from two months to one year although dramatic improvements should be seen sooner than that.

The CORI Robotic Surgery System enhances the accuracy and safety of joint replacement surgery.
CORI ROBOTIC KNEE REPLACEMENT SURGERY
The CORI Robotic System enables orthopedic surgeon in performing joint replacement surgeries as in hip and knee joint replacement. The CORI robotics system uses 3-dimensional intraoperative software that enables the orthopedic surgeon to map out the joint replacement surgery with greater precision and install the artificial joint with much greater accuracy than the human eye.
The new robotic surgery systems provide the surgeon the power of the computer to precisely shape the joint space and place the artificial joint implant into the ideal position during surgery. The robotic technology not only improves the outcomes from joint replacement but also reduces the amount of time the patient is under anesthesia or imaging because the joint replacement surgery goes faster.
Mapping out the surgery in advance speeds the surgery the next day, as the robotic arms are preset precisely to a quarter of a millimeter that then enable the surgeon to more precisely install the artificial joint for the ideal fit. The CORI knee robotic system also controls the speed at which surgical screws or plates are installed creating the ideal speed of rotation.
While using robotic technology requires extensive training, the benefits for the patient are huge as surgery goes much faster. This means that the patient is spending less time under anesthesia and less time under fluoroscopy. The CORI robotic surgery system also often enables the orthopedic surgeon to operate through a smaller incision so the patient has less blood loss, less tissue disruption and less pain as they go through rehab and therapy. Some patients with robotic surgery go home later the same day rather than spending days in the hospital. Consequently, these patients are typically back to activity much faster than with traditional joint replacement surgery.